Guillain-Barré syndrome (GBS): a life-threatening neuromuscular emergency with a rapid, devastating onset compounded by long-term, life-altering consequences1-5
GBS can strike anyone, anywhere, causing paralysis, respiratory failure, and even death2,5,6
Without immediate intervention, patients face continued neuroinflammation and peripheral nerve damage caused by GBS that leads to muscle weakness or paralysis, with lifelong residual deficits impacting their health and quality of life.4,6,7
1 in 3
patients with GBS requires ICU admission8*
Of patients who are hospitalized,
1 in 4
requires mechanical ventilation9†
* From Dhar R et al, "The morbidity and outcome of patients with Guillain-Barré syndrome admitted to the intensive care unit."8
† From Harms M, "Inpatient management of Guillain-Barré syndrome," a review of key issues in inpatient GBS management, which states that the percentage of patients with GBS requiring mechanical ventilation depends on study methodology and ranges from 25% to 44%.9
“I was terrified; there was so much chaos around me as I was put in the ICU and told my body was paralyzed by this disease and that I would likely require a respirator to help me breathe.”
—Patient with GBS
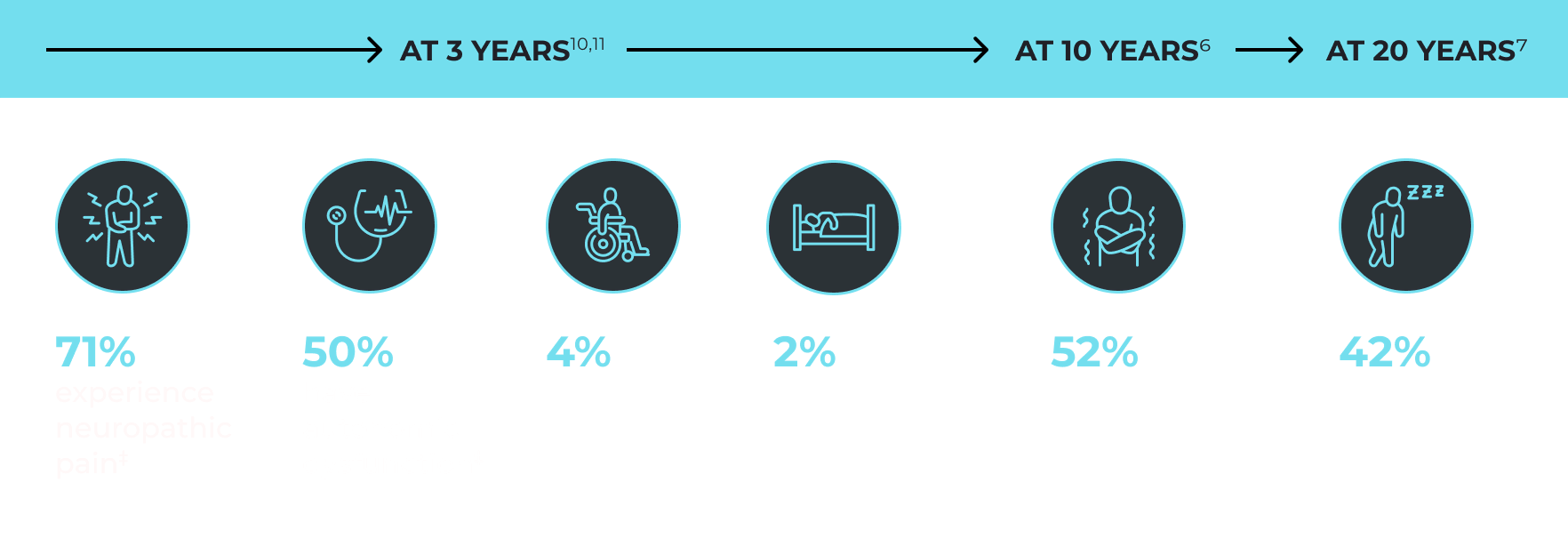
The hidden and residual symptoms of GBS
Residual disabilities make an impact on patients’ social lives and activities of daily living.
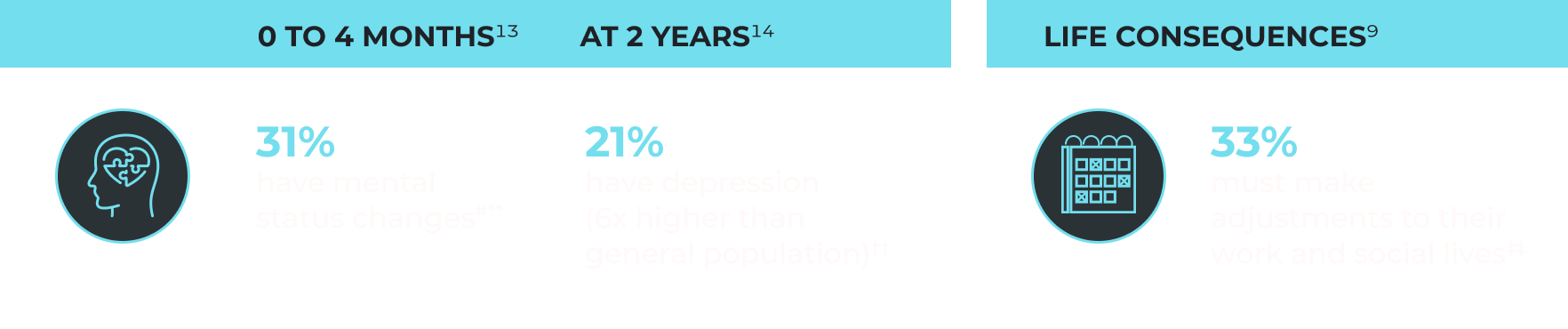
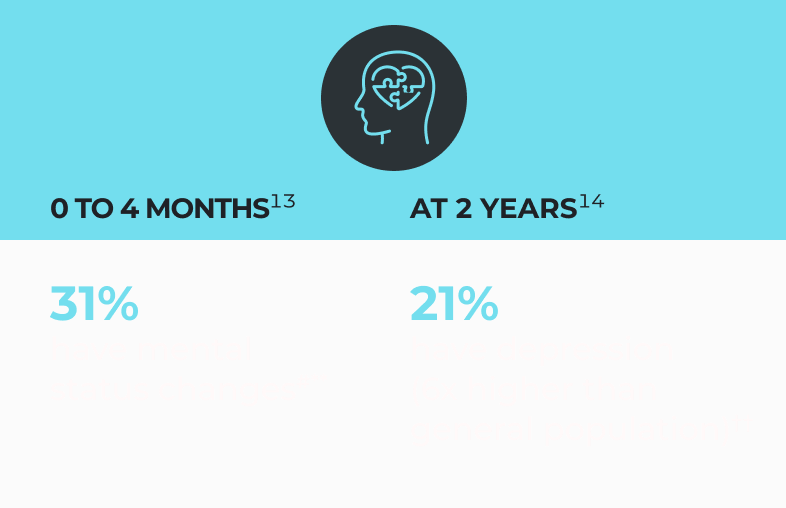
Mental health and psychosocial problems can impact recovery and persist after physical symptoms improve.12
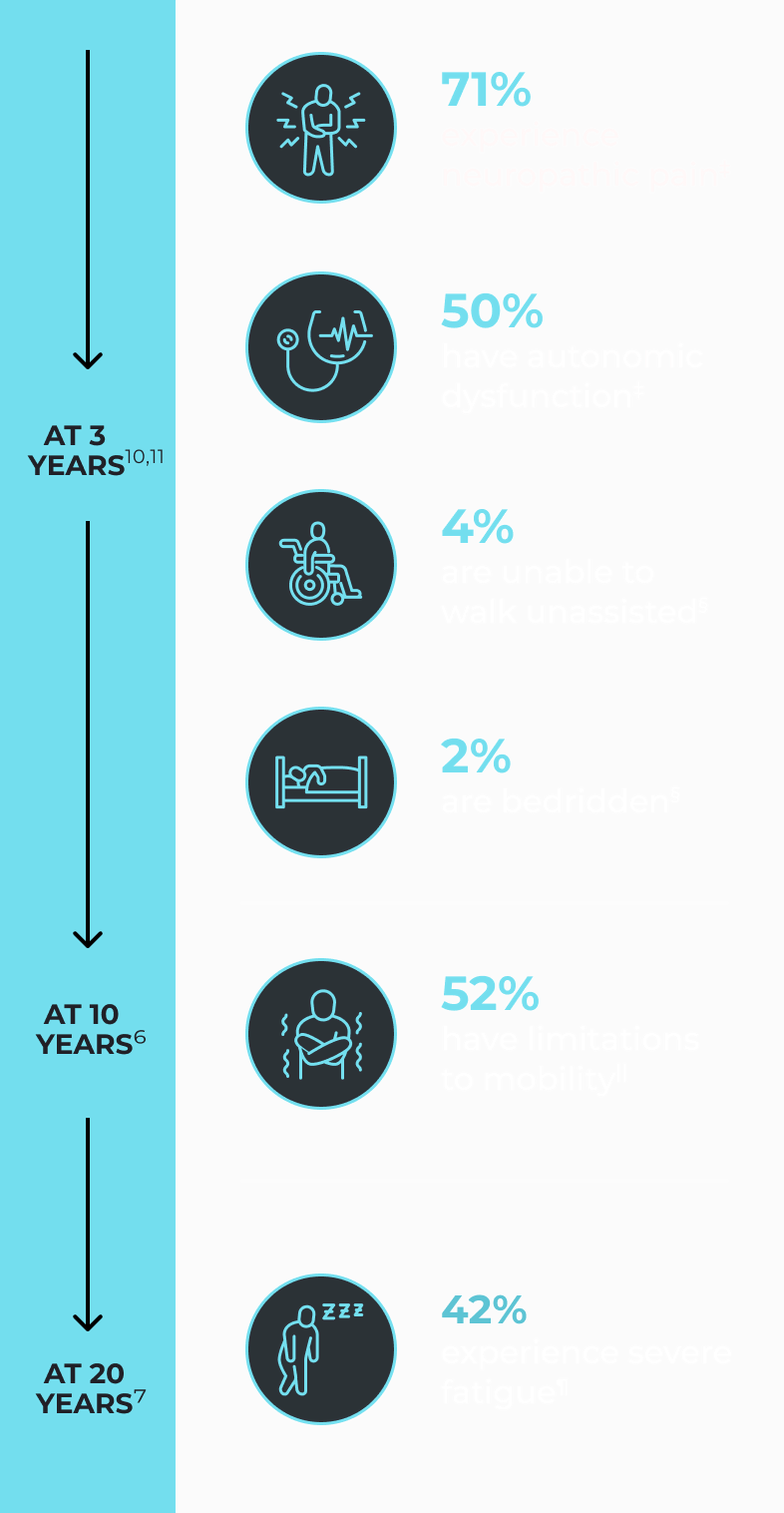
‡ A 3-year follow-up of 24 patients with GBS who received inpatient physical therapy within a 4-year period.10
§ A 3-year follow-up in 54 patients with GBS who were hospitalized in 7 healthcare centers.11
|| A 10-year follow-up in 29 patients with GBS identified from 8 hospitals who were previously followed for 2 years.6
¶ 24 patients who had been admitted to inpatient hospital rehabilitation over a 17-year period were interviewed by a physician experienced in neurological rehabilitation.7
# Eg, vivid dreams, illusions, hallucinations, and delusions.13
** A prospective study of mental status abnormalities in 139 patients with GBS and 55 patients in a control group over a 14-year period.13
†† A population-based analysis of depression diagnoses and/or new prescriptions for anti-depressant drugs in 853 patients with GBS and 8,639 individuals from the general population over 12 years.14
‡‡ From Harms M, "Inpatient management of Guillain-Barré syndrome," a review of key issues in inpatient GBS management.9
“I had to learn how to crawl just like a baby. It took about 2.5 years to learn how to walk. Then I had 5 years of physical therapy.”
—Patient with GBS
Delays in diagnosis can hamper timely treatment and recovery
- Early diagnosis and prompt treatment is essential for improved outcomes4,15,16
- Patients not suspected of GBS at initial evaluation are more likely to require intubation and to have residual weakness at the time of discharge17
- Prompt, accurate diagnosis of GBS requires understanding the heterogeneity of its presentation and being familiar with its pitfalls1,18
Despite current treatment options, recovery can take months or even years3,6,7,9,19-21
There are currently no FDA-approved treatments specifically indicated for GBS.
Intravenous immunoglobulins (IVIgs) and plasma exchanges are commonly used while evidence of their effectiveness is limited.
- 41% of patients receiving IVIg continued to experience residual symptoms, including pain, sensory deficits, and limb weakness, at 1 year in an observational, prospective cohort study of 148 patients who received IVIg and 40 patients who did not
- Despite either treatment, patients remain at risk for respiratory failure, autonomic dysfunction, thromboembolic disease, pain, and psychiatric disorders
The role of the complement pathway in GBS4,22,23
- Antibodies generated against the antecedent infection cross-react with a range of glycolipids in myelin and axonal membrane
- Antibodies bound to nerve cells activate complement
- Complement activation causes neuroinflammation, nerve damage, and destruction leading to common manifestations of GBS—functioning as a common pathway across all GBS types
Research is being done to see whether disrupting the complement pathway may stop further neuroinflammation and tissue destruction in GBS.
Stay up to date on GBS with the latest news from Annexon
Sign up to receive updates and help move GBS forward.
By providing my email address, I am consenting to receive email updates from Annexon, Inc. I understand that I may withdraw my authorization by emailing privacy@annexonbio.com or following the unsubscribe instructions on the communication.
References: 1. Leonhard SE, Mandarakas MR, Gondim FAA, et al. Diagnosis and management of Guillain-Barré syndrome in ten steps. Nat Rev Neurol. 2019;15(11):671-683. 2. Doets AY, Verboon C, van den Berg B, et al. Regional variation of Guillain-Barré syndrome. Brain. 2018;141(10):2866-2877. 3. Fletcher DD, Lawn ND, Wolter TD, Wijdicks EFM. Long-term outcome in patients with Guillain-Barré syndrome requiring mechanical ventilation. Neurology. 2000;54(12):2311-2315. 4. Bellanti R, Rinaldi S. Guillain-Barré syndrome: a comprehensive review. Eur J Neurol. 2024;31(8):e16365. 5. Netto AB, Taly AB, Kulkarni GB, Rao UG, Rao S. Mortality in mechanically ventilated patients of Guillain Barré Syndrome. Ann Indian Acad Neurol. 2011;14(4):262-266. 6. Forsberg A, Press R, Holmqvist LW. Residual disability 10 years after falling ill in Guillain-Barré syndrome: a prospective follow-up study. J Neurol Sci. 2012;317(1-2):74-79. 7. Drory VE, Bronipolsky T, Bluvshtein V, Catz A, Korczyn AD. Occurrence of fatigue over 20 years after recovery from Guillain–Barré syndrome. J Neurol Sci. 2012;316(1-2):72-75. 8. Dhar R, Stitt L, Hahn AF. The morbidity and outcome of patients with Guillain-Barré syndrome admitted to the intensive care unit. J Neurol Sci. 2008;264(1-2):121-128. 9. Harms M. Inpatient management of Guillain-Barré syndrome. Neurohospitalist. 2011;1(2):78-84. 10. Uz FB, Uz C, Karaahmet OZ. Three-year follow-up outcomes of adult patients with Guillain-Barré Syndrome after rehabilitation. Malawi Med J. 2023;35(3):156-162. 11. Martic V, Bozovic I, Berisavac I, et al. Three-year follow-up study in patients with Guillain-Barré syndrome. Can J Neurol Sci. 2018;45(3):269-274. 12. Akanuwe JNA, Laparidou D, Curtis F, Jackson J, Hodgson TL, Siriwardena AN. Exploring the experiences of having Guillain-Barré syndrome: a qualitative interview study. Health Expect. 2020;23(5):1338-1349. 13. Cochen V, Arnuff I, Demeret S, et al. Vivid dreams, hallucinations, psychosis and REM sleep in Guillain-Barré syndrome. Brain. 2005;128(Pt 11):2535-2545. 14. Levison LS, Thomsen RW, Andersen H. Increased risk of depression after Guillain-Barré syndrome. Muscle Nerve. 2023;67(6):497-505. 15. Walling AD, Dickson G. Guillain-Barré syndrome. Am Fam Physician. 2013;87(3):191-197. 16. Min YG, Hong YH, Rajabally YA, Sung JJ. Timing of intravenous immunoglobulin treatment and outcome in Guillain-Barré syndrome: is time nerve? Muscle Nerve. 2024;70(6):1215-1222. 17. Dubey D, Kapotic M, Freeman M, et al. Factors contributing to delay in diagnosis of Guillain-Barré syndrome and impact on clinical outcome. Muscle Nerve. 2016;53(3):384-387. 18. Kenan G, Regev T, Kushnir M, et al. Reasons for delayed treatment initiation in Guillain-Barré syndrome. J Neurol Sci. 2022;434:120179. 19. Guillain-Barré syndrome. National Institute of Neurological Disorders and Stroke. Updated January 31, 2025. Accessed February 28, 2025. https://www.ninds.nih.gov/health-information/disorders/guillain-barre-syndrome 20. Liu S, Dong C, Ubogu EE. Immunotherapy of Guillain-Barré syndrome. Hum Vaccin Immunother. 2018;14(11):2568-2579. 21. Verboon C, Harbo T, Cornblath DR, et al. Intravenous immunoglobulin treatment for mild Guillain-Barré syndrome: an international observational study. J Neurol Neurosurg Psychiatry. 2021;92(10):1080-1088. 22. van den Berg B, Walgaard C, Drenthen J, Fokke C, Jacobs BC, van Doorn PA. Guillain-Barré syndrome: pathogenesis, diagnosis, treatment and prognosis. Nat Rev Neurol. 2014;10(8):469-482. 23. van Doorn PA, Van den Bergh PYK, Hadden RDM, et al. European Academy of Neurology/Peripheral Nerve Society Guideline on diagnosis and treatment of Guillain-Barré syndrome. Eur J Neurol. 2023;30(12):3646-3674.